Associations of Life-Sustaining Treatment–Related Knowledge, Role Perception, and Nursing Stress with End-of-Life Nursing Care Performance among Intensive Care Unit Nurses
Article information

Abstract
Background
This study examined the associations of intensive care unit (ICU) nurses’ knowledge of life-sustaining treatment (LST), role perception regarding LST, and nursing stress related to LST with their performance of end-of-life nursing care.
Methods
A total of 179 ICU nurses from tertiary general hospitals participated in this descriptive correlational study. Data were collected using structured self-administered questionnaires. The data were analyzed using the independent t-test, one-way ANOVA, Mann–Whitney U-test, Kruskal–Wallis test, Pearson’s correlation coefficient, and multiple regression analysis, employing IBM SPSS version 28.0.
Results
The performance of end-of-life nursing care was significantly higher among nurses with 5 to <7 years (β=0.17, P=0.032) and ≥7 years (β=0.20, P=0.011) of total clinical experience, as well as those who had performed end-of-life nursing care 20 times or more (β=0.17, P=0.014). Higher role perception regarding LST (β=0.27, P<0.001) and lower nursing stress related to LST (β=–0.41, P<0.001) were also associated with better performance. These variables explained 31.3% of the variance in end-of-life nursing care performance.
Conclusions
These findings suggest that tailored educational and support programs based on clinical experience and care exposure may be helpful for supporting end-of-life nursing care performance among ICU nurses. In particular, role perception regarding LST and nursing stress related to LST may be important considerations when designing strategies to support the quality of end-of-life nursing care. Such strategies may also contribute to patient dignity and family-centered supportive care in ICU end-of-life situations.
INTRODUCTION
Advances in medical technology have increased medically futile life-sustaining treatment (LST), intensifying debate on death with dignity [1]. LST includes interventions such as cardiopulmonary resuscitation, dialysis, chemotherapy, and mechanical ventilation that may prolong the dying process without reasonable expectation of therapeutic benefit at the end of life [2]. In South Korea, the Act on Hospice and Palliative Care and Decisions on LST for Patients at the End of Life was enacted in 2016 and implemented in 2018 to protect human dignity, promote patients’ best interests, and respect self-determination [2].
Patients admitted to the intensive care unit (ICU) often face decisions regarding the withdrawal or withholding of LST [3]. The ICU is a specialized unit providing intensive monitoring, treatment, and nursing care for critically ill patients [4]. Because mortality is higher in this setting, end-of-life situations occur more frequently than in other departments, and ICU nurses frequently perform end-of-life nursing care [5]. Nursing care related to LST refers to the care provided to patients who are receiving such treatment, and it is conceptually distinct from end-of-life nursing care or hospice care [3]. Limited LST education in nursing curricula and clinical practice has led to insufficient LST knowledge; consequently, ICU nurses often experience difficulty providing appropriate LST-related care [6]. Nurses who care for patients at the end of life must possess sufficient knowledge about LST decisions, to provide accurate information and deliver appropriate end-of-life nursing care [6]. Thus, assessing ICU nurses’ level of LST knowledge and its association with end-of-life nursing care performance for patients receiving such treatment is necessary.
Nurses should not view LST withdrawal as merely the cessation of medical interventions but should integrate the LST decision-making process with end-of-life nursing care to ensure a death with dignity [7] and play a supportive role during the terminal stage after LST decisions [5]. According to previous research [5], a clearer role perception regarding LST is associated with a higher level of performance in end-of-life nursing care. Therefore, it is necessary to investigate ICU nurses’ role perception regarding LST and its association with the performance of end-of-life nursing care.
ICU nurses care for both general patients and those receiving LST without differentiating between them, often experiencing ethical dilemmas during LST continuation or withdrawal and psychological burdens from heavy workloads and advanced facilities and equipment [3]. Nursing stress related to LST may be associated with ICU nurses’ performance of end-of-life nursing care [8]. However, studies report inconsistent associations between LST-related nursing stress and end-of-life nursing care performance [7,9]: general-hospital studies reported a significant negative correlation [7], whereas ICU-nurse research found no significant correlation [9]. Replication studies are needed to clarify this relationship.
Although previous studies have explored LST-related or end-of-life care issues among nurses, many have focused primarily on general hospital nurses [7] or examined selected factors related to end-of-life care performance among ICU nurses [3,8,9]. Furthermore, findings regarding the association between LST-related nursing stress and end-of-life care performance have remained inconsistent [7,9]. This study is distinctive in that by simultaneously investigating these modifiable factors within the ICU, emphasizing the potential role of psychological variables alongside clinical knowledge. In the ICU, appropriate end-of-life nursing care supports patient dignity and family-centered care [2,4], and may contribute to a more health-promoting care environment. By identifying specific modifiable nursing-related factors associated with care performance, this study provides practical evidence for developing targeted support strategies.
Therefore, this study aimed to investigate whether ICU nurses’ LST-related knowledge, role perception, and nursing stress were associated with their performance of end-of-life nursing care, and to provide foundational data to inform the development of tailored end-of-life nursing care programs.
METHODS
Study design
This study employed a descriptive correlational design to identify factors associated with the performance of end-of-life nursing care among ICU nurses.
Participants
The participants of this study were nurses working in ICUs of tertiary general hospitals.
The inclusion criteria were as follows:
(1) nurses currently working in the ICUs of tertiary general hospitals; (2) nurses who have experience providing end-of-life nursing care for patients receiving or withdrawing LST; and (3) nurses who understood the purpose of the study and voluntarily agreed to participate.
The exclusion criteria were as follows:
(1) nurses with less than 1 year of ICU work experience, and (2) nurse managers who do not directly provide end-of-life nursing care.
Nurses with less than 1 year of ICU experience were excluded because they generally have a lower understanding of the meaning of death and higher death anxiety, resulting in an underdeveloped perception of death [5]. Nurse managers were also excluded because they are not directly involved in providing end-of-life nursing care.
Using G*Power version 3.1.9.2, the required sample size for multiple regression analysis was calculated with a significance level (α) of 0.05, a power (1–β) of 0.95, an effect size of 0.15, and 16 predictor variables. The minimum required sample size was 143 participants. Considering a potential dropout rate of 20%, data were collected from a total of 179 ICU nurses, and all 179 completed questionnaires were included in the final analysis.
Measures
General characteristics
General characteristics included age, sex, marital status, religion, highest education level, total work experience, ICU work experience, working department, participation in LST education, participation in end-of-life nursing education, and the number of end-of-life nursing care experiences within the past year. Based on a clinical ladder framework for nurses in tertiary hospitals, total work experience and ICU work experience were categorized into 1–<3, 3–<5, 5–<7, and ≥7 years [10]. Because nurses with less than 1 year of ICU experience were excluded from this study, the <1 year category in the original framework was not applied. The number of end-of-life nursing care experiences within the past year was categorized into <10, 10–<20, and ≥20 times based on a previous nursing study [11].
Knowledge of life-sustaining treatment
Knowledge of LST was measured using the instrument developed by Kim [12]. The tool consists of 16 items answered with “yes,” “no,” or “don’t know.” Correct answers were scored as 1 point, and incorrect or “don’t know” responses were scored as 0. Total scores range from 0 to 16, with higher scores indicating greater knowledge of LST. Reliability was Kuder–Richardson 20 (KR-20)=0.63 in Kim’s study [12] and KR-20=0.72 in this study.
Role perception regarding life-sustaining treatment
Role perception regarding LST was assessed using the scale developed by Byun et al. [13]. The instrument comprises 13 items rated on a 5-point Likert scale, ranging from 1 (“strongly disagree”) to 5 (“strongly agree”). Twelve items are positively worded and one item is negatively worded. Higher scores represent a higher level of role perception regarding LST. Reliability was Cronbach’s α=0.88 in Byun et al.’s study [13] and Cronbach’s α=0.82 in this study.
Nursing stress related to life-sustaining treatment
Nursing stress related to LST was measured using the tool developed by Lee and Kim [3]. This instrument consists of 28 items rated on a 5-point Likert scale, ranging from 1 (“strongly disagree”) to 5 (“strongly agree”). Higher scores indicate greater nursing stress related to LST. Reliability was Cronbach’s α=0.93 in Lee and Kim’s study [3] and Cronbach’s α=0.90 in this study.
Performance of end-of-life nursing care
Performance of end-of-life nursing care was measured using the instrument developed by Park and Choi [14] and revised by Choi [15]. The tool includes 18 items rated on a 4-point Likert scale, ranging from 1 (“never”) to 4 (“always”). It consists of three subdomains: physical (7 items), psychological (8 items), and spiritual (3 items). Higher scores indicate greater performance of end-of-life nursing care. Reliability was Cronbach’s α=0.85 in Choi’s study [15] and Cronbach’s α=0.81 in this study.
Data collection
Data were collected from October 20 to November 10, 2023, from nurses working in ICUs of tertiary general hospitals in South Korea. Data were collected using an online self-administered survey. Recruitment announcements describing the purpose of the study and inclusion criteria were posted on an online nurse-exclusive community platform (Naver Cafe: Meeting Representing Nurses). Nurses who met the eligibility criteria and voluntarily agreed to participate were recruited through convenience sampling. Participants accessed the questionnaire via an online survey link and completed the survey anonymously. In addition, a snowball sampling method was employed, whereby participants were encouraged to share the survey link with other eligible ICU nurses. Completing the questionnaire required approximately 15–20 minutes, and participants received a small token of appreciation for their time and participation.
Data analysis
Data were analyzed using SPSS/WIN version 28.0 (IBM Corp.). General characteristics of participants were analyzed using frequencies, percentages, means, standard deviations, medians, and interquartile ranges. The levels of knowledge of LST, role perception regarding LST, nursing stress related to LST, and performance of end-of-life nursing care were analyzed using descriptive statistics (mean and standard deviation). Differences in the performance of end-of-life nursing care according to participants’ general characteristics were analyzed using the independent t-test, one-way analysis of variance (ANOVA), Mann–Whitney U-test, and Kruskal–Wallis test, with post-hoc comparisons performed using the Mann–Whitney U-test. Correlations among knowledge of LST, role perception regarding LST, nursing stress related to LST, and performance of end-of-life nursing care were examined using Pearson’s correlation coefficient. Finally, a multiple regression analysis (enter method) was conducted to identify factors associated with the performance of end-of-life nursing care. Total work experience and end-of-life nursing experience, which showed significant differences in end-of-life nursing care performance in the univariate analyses, were entered as control variables. Knowledge of LST, role perception regarding LST, and nursing stress related to LST were entered as the main independent variables. Model adequacy was evaluated by examining the independence of residuals and multicollinearity.
Ethical considerations
This study was approved by the Institutional Review Board (IRB) of Jeonbuk National University (IRB No. JBNU 2023-09-002-001) and adhered to the Declaration of Helsinki. Participants were recruited online after receiving detailed information regarding the study’s purpose, voluntary participation, and the right to withdraw without penalty. Informed consent was obtained electronically, ensuring strict anonymity and confidentiality. All personal contact information collected for compensation was securely deleted upon distribution.
RESULTS
General characteristics of participants
The participants’ mean age was 29.63±3.50 years, with a majority being in their 20s (59.2%), female (86.0%), and unmarried (57.5%). Most held an associate or bachelor’s degree (87.2%) and reported having no religion (77.1%). The mean total clinical and ICU experience were 5.39±3.18 and 4.39±2.28 years, respectively, with the medical ICU (40.2%) being the most common working unit. Regarding specialized education, 31.8% had received LST-related training, and 42.5% had received end-of-life care education. Over the past year, participants performed end-of-life nursing care an average of 10.46±4.97 times, with the majority (63.1%) experiencing 10 to fewer than 20 cases (Table 1).

Differences in performance of end-of-life nursing care according to general characteristics of participants (n=179)
Levels of knowledge, role perception, and nursing stress related to life-sustaining treatment, and performance of end-of-life nursing care among intensive care unit nurses
Mean scores for LST knowledge, role perception, and nursing stress were 12.71±2.82, 4.29±0.42, 4.30±0.43, respectively. Performance of end-of-life nursing care averaged 2.96±0.32.
Differences in intensive care unit nurses’ performance of end-of-life nursing care according to general characteristics
There were significant differences in the performance of end-of-life nursing care according to total work experience (F=3.36, P=0.020) and the number of end-of-life nursing care experiences (H=11.51, P=0.003) among ICU nurses. Post hoc tests showed that nurses with ≥7 years of total work experience (3.05±0.21) demonstrated higher levels of performance of end-of-life nursing care than those with less than 3 years (2.85±0.28). Additionally, nurses with 20 or more end-of-life nursing care experiences (3.17±0.26) showed higher performance of end-of-life nursing care compared to those with fewer than 10 experiences (2.87±0.28) (Table 1).
Relationships among knowledge of life-sustaining treatment, role perception regarding life-sustaining treatment, nursing stress related to life-sustaining treatment, and performance of end-of-life nursing care
The performance of end-of-life nursing care showed a significant positive correlation with knowledge of LST (r=0.18, P=0.018) and role perception regarding LST (r=0.27, P<0.001), and a significant negative correlation with nursing stress related to LST (r=–0.40, P<0.001) (Table 2).

Relationships among knowledge of LST, role perception regarding LST, nursing stress related to LST, and performance of end-of-life nursing care (n=179)
Factors associated with the performance of end-of-life nursing care among participants
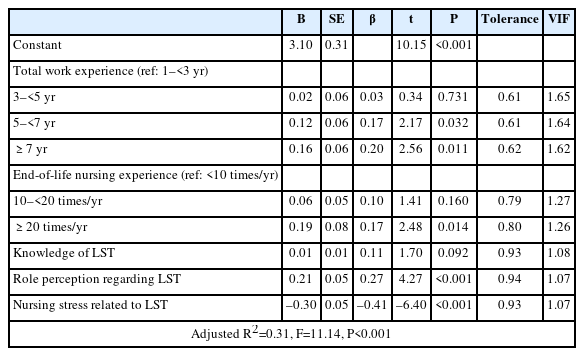
To identify factors associated with the performance of end-of-life nursing care, total work experience and end-of-life nursing experience were entered as control variables, while knowledge of LST, role perception regarding LST, and nursing stress related to LST were entered as the main independent variables. Total work experience and end-of-life nursing experience were treated as dummy variables, and the enter method was used for variable selection. Assumptions for regression were met, with no autocorrelation (Durbin–Watson=2.00) or multicollinearity (tolerance, 0.61–0.94; variance inflation factor, 1.07–1.65) detected.
The overall regression model for the performance of end-of-life nursing care was significant (F=11.14, P<0.001). Compared to nurses with less than 3 years of total work experience, those with 5–<7 years (β=0.17, P=0.032) and ≥7 years (β=0.20, P=0.011) demonstrated higher performance. Additionally, nurses with 20 or more experiences of end-of-life nursing care (β=0.17, P=0.014) showed higher performance compared to those with fewer than 10 experiences. Higher role perception regarding LST (β=0.27, P<0.001) and lower nursing stress related to LST (β=–0.41, P<0.001) were associated with higher performance of end-of-life nursing care. These variables collectively explained 31.3% of the variance in the model (Table 3).
Factors associated with the performance of end-of-life nursing care (n=179)
DISCUSSION
This study identified several factors associated with ICU nurses’ performance of end-of-life nursing care. In the final model, higher role perception regarding LST and lower nursing stress related to LST were significantly associated with better performance, whereas knowledge of LST was not a significant predictor. In addition, nurses with greater total clinical experience and more frequent end-of-life nursing care experience showed higher performance. These findings suggest that, in ICU settings, modifiable psychological and practice-related factors may be more directly relevant to end-of-life nursing care performance than knowledge alone.
The level of end-of-life nursing care performance observed in this study was comparable to that reported in previous studies involving ICU nurses using the same measurement tool [15], and higher than that reported among nurses working in general wards of tertiary hospitals [16]. This pattern may reflect the ICU context, in which nurses more frequently encounter patients who deteriorate despite intensive treatment and require ongoing end-of-life nursing care [8]. Although ICUs are not specialized end-of-life care units, ICU nurses often remain closely involved in caring for critically ill patients throughout the dying process. In this regard, the relatively higher performance observed in this study may suggest that repeated exposure to end-of-life situations in ICU settings contributes to greater familiarity with and responsiveness to end-of-life nursing needs.
In this study, nursing stress related to LST was moderate to high, consistent with findings from previous studies involving ICU nurses in general and tertiary hospitals using the same measurement tool [3,17], and higher than that reported among general ward nurses [18,19]. This pattern may reflect the distinctive ICU environment, where nurses are required to manage critically ill patients, complex LSTs, and rapidly changing clinical situations. In such settings, the need for advanced technical competence and immediate responses to emergencies may intensify psychological burden and emotional exhaustion, thereby increasing LST-related nursing stress [20].
Nursing stress related to LST was significantly associated with end-of-life nursing care performance in this study, though prior findings have been inconsistent [7,9]. This discrepancy may reflect differences in participant characteristics, hospital settings, and model composition. For example, a prior study [9] included nurses from both tertiary and general hospitals with shorter experience requirements, whereas this study focused exclusively on tertiary general hospital ICU nurses with at least 1 year of ICU experience. Moreover, because nursing stress may be shaped by multiple factors [21], its relationship with performance may vary across settings. By focusing specifically on LST-related factors, this study may have captured a more direct association. In ICU settings, where communication surrounding LST decisions may be challenging [19], clearer role delineation, clear and supportive communication, and multidisciplinary collaboration may help reduce LST-related nursing stress and support end-of-life nursing care performance [4,19].
Participants’ role perception regarding LST was comparable to, or slightly higher than, that reported in previous studies involving general hospital nurses [18,19] and ICU nurses [22,23]. In this study, higher role perception regarding LST was significantly associated with better end-of-life nursing care performance. This finding suggests that a clearer understanding of nurses’ roles in the context of LST decision-making may be an important factor supporting end-of-life nursing care performance in ICUs. Previous research has shown that nurses’ active involvement in LST decision-making is important for providing informational and emotional support to patients and families [3]. However, despite the legal framework for LST decisions in South Korea, insufficient role-specific guidance and standardized institutional protocols may still lead to confusion regarding nurses’ roles in practice [24]. Therefore, clear clinical guidelines, systematic education, and support for counseling and advocacy roles may help strengthen nurses’ role perception regarding LST and, in turn, support end-of-life nursing care performance [24,25].
Knowledge of LST was not significantly associated with end-of-life nursing care performance in this study. To our knowledge, few studies have directly examined this association among ICU nurses. One possible explanation is that the knowledge instrument primarily assessed legal and decision-making aspects of LST, whereas end-of-life nursing care performance encompassed physical, psychological, and spiritual domains. This difference in construct coverage may have limited the extent to which LST-related knowledge translated directly into broader end-of-life nursing care performance. In addition, recent ICU research suggests that knowledge relevant to end-of-life care may vary by domain, with psychosocial and spiritual aspects often remaining limited despite overall clinical experience and education [26]. Future studies should therefore use more refined and up-to-date instruments to examine how different domains of LST- and end-of-life care-related knowledge are linked to end-of-life nursing care performance in ICU nurses.
The present study also showed that total work experience and the frequency of end-of-life nursing care experiences were significantly associated with end-of-life nursing care performance, partially differing from previous findings [8]. In particular, nurses with 5 years or more of clinical experience showed higher performance than those with less than 3 years. This may reflect progression in clinical competence and role development across career stages; in a clinical ladder framework for tertiary hospital nurses, the period after 5 years of experience corresponds to more advanced levels of practice characterized by greater ability to manage complex situations and coordinate care [10]. These findings support the need for structured educational support tailored to less experienced nurses, particularly to help them develop confidence and preparedness in providing end-of-life nursing care.
From a health-promotion perspective, strengthening nurses’ role perception regarding LST and reducing LST-related nursing stress [3,18] may help foster a more supportive end-of-life care environment in ICUs [24]. Such efforts may also better support patients and families during the dying process.
This study has several limitations. First, because participants were recruited through convenience and snowball sampling, the sample may not be fully representative of ICU nurses in South Korea, which limits the generalizability of the findings. Second, the instrument used to measure knowledge of LST showed modest internal consistency. Because this scale is composed of dichotomously scored items, its KR-20 may be relatively modest compared with that of instruments with more response categories, even when the number of items is the same [27]. Nevertheless, this remains a limitation of the present study, and further refinement and validation of the instrument are needed. In addition, self-reported data may be subject to social desirability bias, and the use of structured instruments may not fully capture the complexity of clinical practice. Future research should employ more diverse and representative sampling methods, use objective data collection approaches, and further validate measurement tools.
In conclusion, role perception regarding LST, nursing stress related to LST, and clinical experience were associated with ICU nurses’ performance of end-of-life nursing care. Nurses with at least 5 years of experience and frequent end-of-life encounters showed higher performance. These findings suggest that structured and continuous support programs tailored to less experienced nurses, particularly those addressing role perception, communication, and LST-related stress, may be useful for supporting the quality of end-of-life nursing care and fostering a more health-promoting care environment in ICUs.
Notes
AUTHOR CONTRIBUTIONS
Dr. Jihyun BAEK had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. All authors reviewed this manuscript and agreed to individual contributions.
Conceptualization: SM and JB. Data curation: SM and JB. Formal analysis: SM and JB. Investigation: SM and JB. Methodology: SM and JB. Project administration: JB. Resources: SM and JB. Supervision: JB, JHK, and HYK. Validation: all authors. Visualization: SM and JB. Writing–original draft: SM and JB. Writing–review & editing: all authors.
CONFLICTS OF INTEREST
Jeong Hee KANG is the Editor of this journal and was not involved in the peer review or editorial decision-making process for this article. No other potential conflicts of interest relevant to this article were reported.
FUNDING
None.
DATA AVAILABILITY
The dataset supporting the conclusions is available from the corresponding author on reasonable request.
ACKNOWLEDGMENTS
This article is based on a part of the first author’s master’s thesis from Jeonbuk National University.
We thank all participants for their voluntary participation. The authors used ChatGPT (OpenAI) to refine the language for clarity and readability. The authors take full responsibility for the content.